
Preparation
It’s always good to be prepared. It gives you something to do and you will feel more in control of the situation. You will need:
- very large sanitary pads and a decent number of them
- a container to put the baby in
- absorbent under pads (chux)
- at least one old towel
- scissors (just in case)
- something to drink
- cold washcloth (for you)
- (optional) strainer to use while on the toilet
I recommend the chux because 1) there will be a lot of blood – (it’s easier to use the chux (they have a water-proof backing) and throw them away) and 2) there will be a good number of sizable blood clots and the placenta and the chux are convenient for disposing of them neatly.
*Note: Although it is perfectly possible to undergo a natural miscarriage on your own, if you are more than a few weeks along it is advisable to have someone else in the house with you, if not in the same room. At best you will have moral support and at least you will have someone to call on in an emergency. If it is unavoidable that you are alone, have a phone within reach in case of emergency.
Signs of impending miscarriage
- cramping, period cramps or harder, sometimes approximating labor pains
- spotting – will probably start brownish and then turn red
- sometimes an upset stomach
Sometimes you will simply be surprised. If this happens it is at least likely to be quick. If you notice any signs of spotting or just ‘have a feeling’ it’s coming, go ahead and assemble your supplies and if you are alone, call someone to be with you. I advise putting a pad on and/or a chux under you. When the bleeding starts in earnest, it is very likely to be sudden and dramatic.
Managing the actual miscarriage
If you have been waiting for a while to miscarry, as in the case of a missed miscarriage, then you may be relieved to have the process finally starting. You may also be overwhelmed with grief or panic. Keep in mind that women have been miscarrying at home for thousands of years. This is where having a support person can be very helpful. Take a deep breath and say a prayer. If it helps, place an icon where you can see it.
On dry land:
If you are most comfortable on your bed or the floor (I don’t recommend the couch), then you will be very, very glad that you have chux available. It is a good idea to put down a layer of four or more chux so that one can be removed easily and another one waiting. There is no scripted position. Sit, crouch, kneel, whatever. The position that makes you the most comfortable is likely to change throughout. Do whatever feels better. Do be in a position that you have something to lean back against if you need to. This can be another person. You may feel faint at some point and need the support.
In water:
Most women find warm water eases the pain associated with cramps and the water helps support your weight so positions are easier to hold. The water may be psychologically helpful because after a very few minutes the water is mostly opaque and you cannot immediately see anything you’re not ready to see. The bathtub also provides a natural backrest and handholds. Changing positions when in the tub is the same as on dry land. When you are done delivering everything you can clean up right in the tub instead of transferring. Place a few chux on the floor next to the tub so you can keep everything tidy when you get out (and to provide a place to put things if necessary).
On the toilet:
Some women find this position to be most comfortable. I recommend having a strainer in place so you don’t have to retrieve the baby from the toilet – this can be emotionally painful. The advantage is that you can flush the clots rather than having to dispose of them otherwise. I do not recommend flushing the placenta unless it is fairly small. At between 12 and 13 weeks of growth my placenta was easily 9 inches across and thick. If you start to feel faint while on the toilet, then quickly move to the bathroom floor. Better that than to fall. Place a chux or two on the floor under your feet.
(From here on out everything is the same regardless of your chosen position.)
My first miscarriage began with a sudden rush of blood (after initial cramping and spotting for a few hours). Very soon after that I delivered the amniotic sac (containing the baby) and a large clot. You may pass several clots first.
After delivering the baby feel free to “stop” and hold him. If he is in the sac, carefully open it up.** Having wet hands helps hold the baby because of his fragile skin. Take some time to hold him and talk to him. You are not in any hurry here. When you are ready, place him in the container (I suggest having water or saline in it) so you can finish passing everything. One reader asked that I note that if you want to rinse something off, it is better to “swish” the sac/baby/placenta/tissue in a container of water rather than run the tap over it due to the delicacy of what you’re handling. You can also take advantage of the container of water/saline to hold the baby in your hand while it is submerged in the water. At least one example of this is on the photographs page.
It may happen that when you deliver the sac you notice the cord is still attached. Don’t pull on it; go ahead and cut it (there’s no need to tie it off).


** Depending on how long it has been since the baby died, you may see something different in terms of the sac. Usually the amount of amniotic fluid decreases over time so depending on how much there was to start with, you may or may not see a nice, full “bubble”. In addition (and this is important), the uterus will form a clot around the sac/baby as time goes on. This means that you may deliver the baby in the sac very obviously, or you may deliver a sac with a clot attached, or you may deliver what appears to be a large clot or placenta but which is actually the sac enclosed in a clot. Especially if you feel as though you are completing the miscarriage but haven’t seen the sac, check inside the large clots. This sounds gross, but it will feel a little different when you are looking for your baby. The clot will be on the sac, not the baby (all things being equal) so you will still be able to remove the baby from the sac if you so desire. When my first son was born his sac had a large clot attached. It covered about 1/3 of the surface. When my second son was born there was no clot attached at all.
For example, here are some photographs of Thea’s twins. Their amniotic sacs and placenta were surrounded by clot which had to be manipulated before the babies came into view.
Thea: “This is what the tissue looked like right after I miscarried:”
“Moving away blood and clots uncovered the gestational sac with placenta attached and some weird tubular-shaped membranous tissue off to the right. I could see two tiny white bodies through the gestational sac.”

“After ripping open the gestational sac the two amniotic sacs came into better view. The sacs were very close together before I spread them apart to take the photo. The tiny babies are inside the sacs, one just above the 10 and 1/4 inch mark and the other just above the 11 inch mark.”
[You can see the rest of the pictures of Thea’s twins on the Photographs page.]
For another example, when Kristen delivered her son, Ryan, at 13 weeks, he was encased in this mass of tissue:

Between the time you deliver the baby and the placenta you are likely to pass several clots and a lot of blood. A word about the blood: Just as you don’t panic when you have a very heavy period, do not panic now. This blood is mostly endometrial lining sloughing off and not directly out of your blood vessels. As the placenta detaches you will have some “active” bleeding, but we’ll talk about that in a moment. The clots are not tissue, they are just that – clots. Whenever blood sits for any time it clots. This is what it is doing inside you. Some will be large, the size of your palm. The blood will be a steady trickle with occasional gushes (as a clot is moved out of the way). If there is a problem later and you need to tell someone how much blood you passed, you will be able to mention the number of chux used. (Yes, this is the one disadvantage of an in-water miscarriage.)
The Placenta
The placenta may come out rather quickly or not. You do not want this to take a long time – say, not much more than an hour. The uterus will not stop bleeding until it is able to tightly clamp down (remember, it’s like a big muscle) and it cannot do that if anything is still inside. Thus, you will continue to bleed and pass clots until the placenta is delivered. If it feels like it’s been a while, you can do something very simple to encourage it to come out. (And, by the way, do not pull on the cord. It won’t work at best and at worst you can cause damage.) You have probably already been able to feel your fundus, the top of the uterus. Find it now and massage it very firmly. Don’t punch yourself, but rub slowly and deeply until you feel strong cramps beginning. Continue to massage for another minute or so to make sure the cramps will continue. The cramps are the uterus contracting to try to expel the placenta. Go by how you feel here, but after a few minutes try bearing down. Do this a few times. If the cramping subsides, massage your fundus some more. This is almost certain to result in the delivery of the placenta in under ten minutes. If more than an hour has gone by, you are still bleeding copiously, and there is no sign of the placenta, consider getting medical assistance. Sometimes placentas are embedded very deeply in the uterine wall and are difficult to expel. We will talk more about when to call for help below.
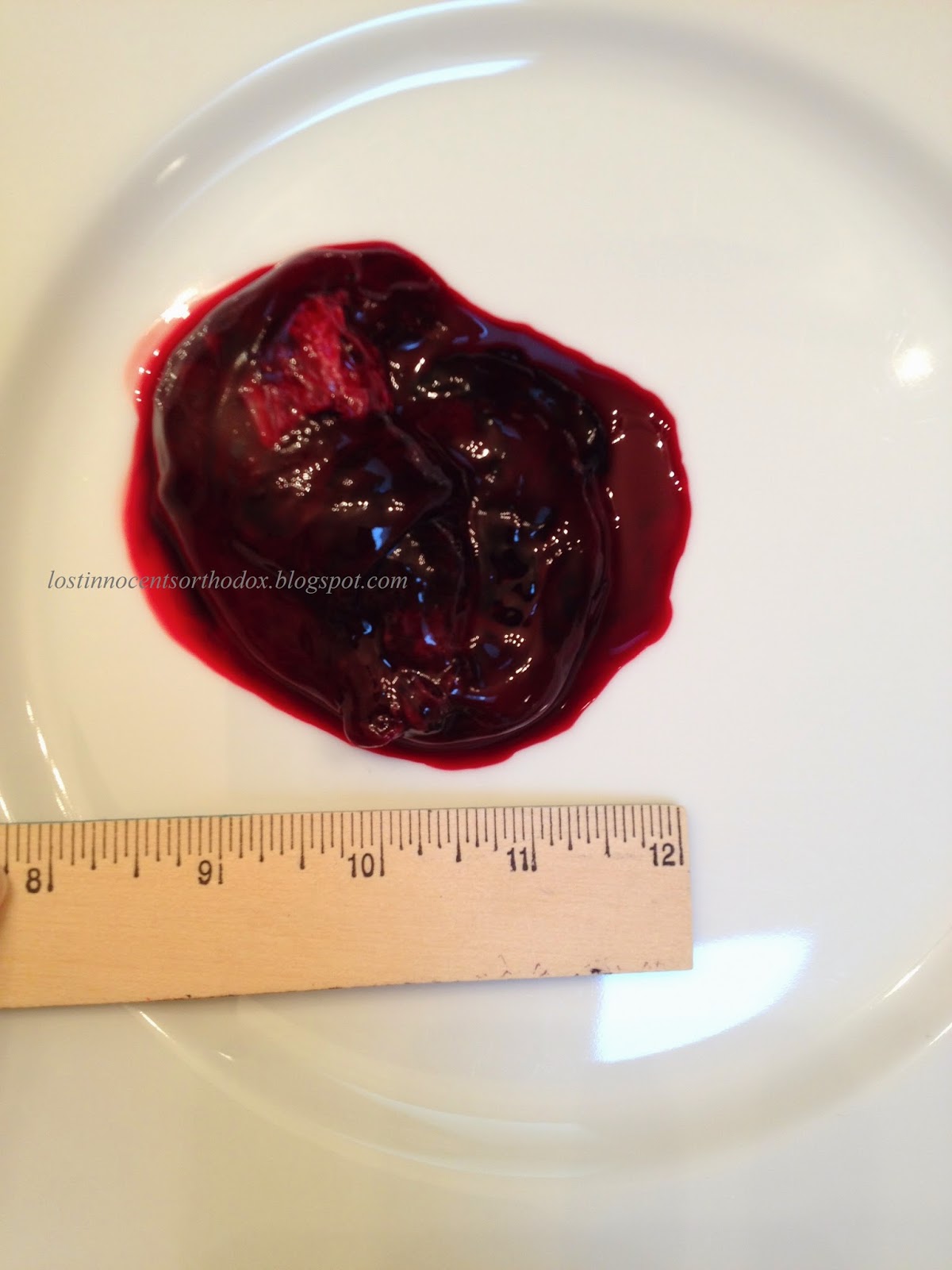
When the placenta is delivered if it is intact you will (hopefully) find it unmistakable. [Reference photos below.] The maternal side (the side that was against the uterine wall) will look like raw hamburger – sorry. The baby’s side will be covered with a shiny “skin” and will look more purplish. Blood vessels will be seen leading toward the umbilical cord in the center. Put the placenta on a chux and have a good look at it. It should be round to ovalish in shape and will vary in size with the length of the pregnancy. There should not appear to be pieces missing from the edge (which would lead one to believe part of the placenta is still in place). If you are not sure what you are looking at, or if the placenta is complete or not, don’t hesitate to put the placenta in a watertight container to take to the doctor. If the placenta does not appear to be complete and if you have not delivered all the pieces, then you will need to seek medical attention. A D&C may have to be done to remove the remaining part(s). Alternately, your placenta may deliver completely but in pieces. You can tell the placenta from the clots because the clots are easily broken up. The placenta will feel more “fibrous”.

Placenta size can vary significantly depending on the length of the pregnancy. In a missed miscarriage the placenta may keep growing for several weeks until the body recognizes that the baby has died. The placenta below is from a baby measuring 6 weeks, 1 day, but not miscarried until 14.5 weeks. (There are more photos on the Photographs page: Selah Lael 6 weeks, 1 day.)

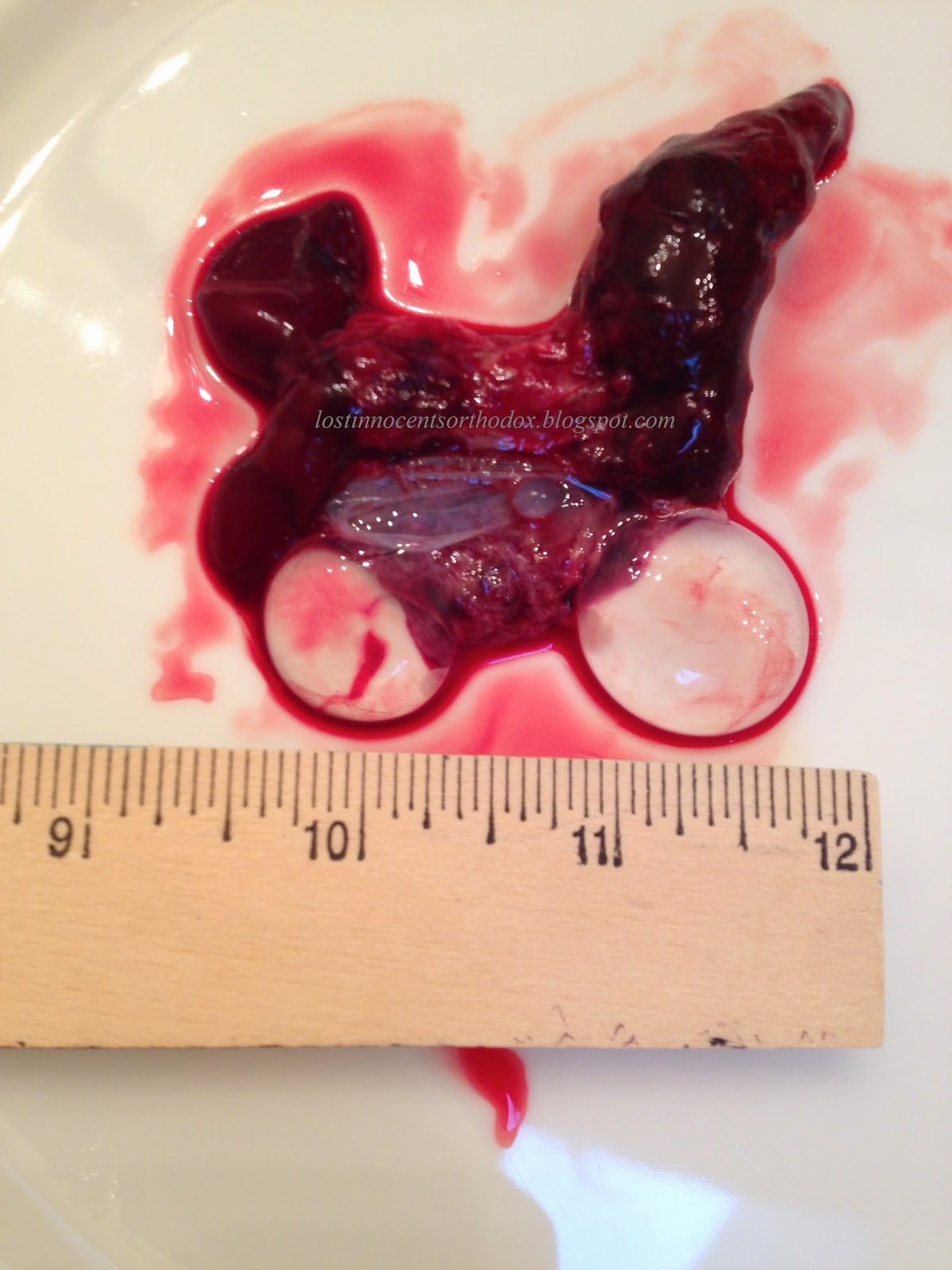
Below is a photograph of a placenta with (collapsed) sac attached (and possibly some clot attached too) generously donated by Allison. Her baby died at 7 weeks and she miscarried at 11 weeks. The doctor confirmed that this is what she was looking at.

Below are two photographs of a placenta from a twin pregnancy. In the first you can see 11 week Arrow on top of the placenta. In the second you can see a gestational sac containing 5 week Cedar on the bottom edge of the placenta. The entire placenta is a little larger than my palm (per other photos with scale context). (You can see additional photos of Cedar and Arrow on the Photographs page.)

Heavenly miscarried again later this year and sent photographs of her baby (Zion) and placenta, shown below.


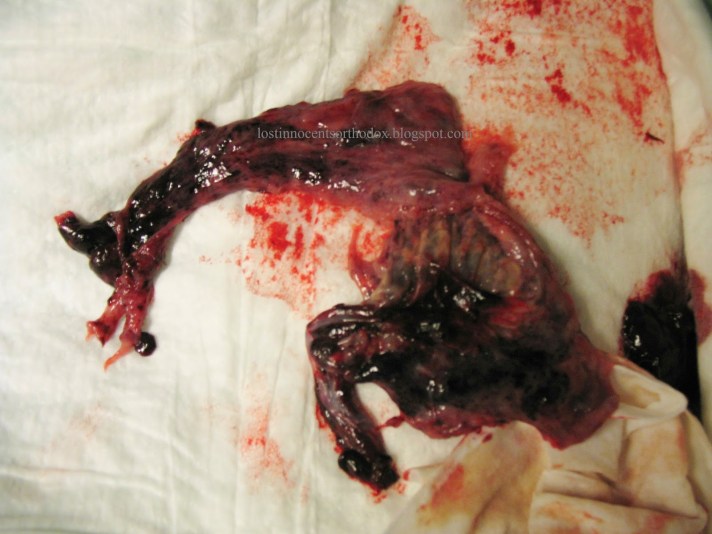
Below are two photographs of the placenta I delivered with my third baby, Gabriel. He died at about 11 weeks and was delivered 19 days later. While the placenta was delivered all at once, it was not intact. It appeared to have torn 80% down the middle. If put back together it would be approximately the area of my hand (5 in x 6 in). (I’m sorry the first photo is a bit blurry. I was pretty faint from blood loss at this point and can’t believe I managed to take pictures at ALL.)

This photograph was just submitted by a woman who delivered her 11 week, 5 day baby in the hospital at 14 weeks, 1 day. You can see the difference between the placenta on the right and the blood clot on the left.



[There are some additional photographs of babies in sacs with or without placentas on the photographs pages.]
After the placenta is delivered you will still pass some more blood, probably a gush behind the placenta, and possibly some more clots. This should decrease quickly after the placenta is out however. The cramping and pain should decrease significantly at this point too. If you are taking something over the counter for pain, take acetaminophen rather than ibuprofen because the latter can increase bleeding.
Afterward
When you are ready, clean up using cool (not cold, unless you want to) water. Warm to hot water will make the blood harder to remove. Put on a pad and lie down. If you have not been sipping all along, drink a full glass of something at this point. You will have lost fluid volume and need to replace it. Do not take this opportunity to clean the entire bathroom. If you do, you will wind up passing out or very nearly (like I did).
At some point I recommend you take photographs of the baby. If you simply can’t do this, have someone else do it. Even if you don’t want to see the pictures now, you will probably want to see them later and it will be nice to have them. Take lots. Take photographs of details. Put wedding rings or something next to the baby for scale. You need never share these photos, but you may wind up treasuring them yourself. After taking photographs, place the container containing the baby in the refrigerator. This slows decomposition.
[Note: After my third loss I was really faint from loss of blood and very exhausted. I left Gabriel in the sac in the container of water. I took a few pictures, but waited until the next afternoon when I was physically more recovered and more emotionally ready to proceed. Don’t feel like you have to rush.]
Recovery
After you miscarry call your doctor. They will almost certainly want to see you for a follow-up ultrasound (to see if the uterus is empty) and an exam. Expect to bleed for about one to two weeks. The pattern may be stop and start. Eventually the discharge will change from red to brown to tan. If the bright red bleeding persists after this, check with your doctor. There may have been something retained in the uterus that was not previously detected. Use pads, don’t use tampons. Do not insert anything into the vagina until you have stopped bleeding. Do not do any heavy labor, strenuous exercise, etc., during the first several days at least. Get extra rest. Make sure you drink enough fluids. Take a few days off from work. Even if you have a desk job, you will probably not feel up to facing anyone yet.
One thing that people are not told to expect is some depression. Obviously, there is the grief from losing your baby, but there are other factors at play. When you deliver, whether at 8 weeks or 40, the hormones that have been very high during pregnancy drop precipitously. This is usually referred to as “the baby blues” and if more severe or persistent, “postpartum depression”. What most people are not aware of is that women who miscarry are at as least as much risk for postpartum depression as women who deliver live babies and usually more. If you have delivered a living baby you will be distracted by the care of a newborn and you will be surrounded by balloons and flowers and congratulations. After a miscarriage you not only do not have these, but you have the added grief of pregnancy loss. Do not hesitate to get help if this is becoming a problem. Pills will not make grief go away, but you may need some support for the physical causes of depression.
When to seek medical attention:
| 1. Fever over 100 degrees F 2. Severe abdominal pain or pain that is increasing (except the normal increasing of cramps until the baby is delivered) 3. Nausea and vomiting (some women experience this during the actual miscarriage – that’s ok) 4. Difficulty urinating 5. Foul-smelling vaginal discharge 6. Bleeding that saturates a pad an hour for more than a few hours straight after everything is expelled. 7. If you think you did not expel everything from the uterus or if the placenta appears to be incomplete. |
Something very important to consider is what to do with your baby after you deliver. I’m not talking about what to do while you’re waiting for burial, I’m talking about taking the baby with you to the doctor’s office or hospital. I strongly recommend that you do not do this. Call ahead to either location before you go (unless it is a genuine emergency, and even then it’s a good idea). If you are planning to take the baby with you, inform the staff that you will be bringing the baby but no one is permitted to touch him and he will remain in your custody. The reason is this: it has come to light that once the hospital takes possession, even for a moment, of your baby, they may refuse to give him back. They may insist on testing. There is no reason for them to do this unless you yourself wish to have testing performed. If you deliver in the hospital, you will automatically be up against this. [Note: I was informed by my doctor’s office after the fact that if anyone brings in the baby after having delivered at home, they are supposed to take the baby to the hospital pathology department. Somehow, they let me get away with bringing my baby in to show them and then returning home with him. Just a word of warning.]
Hospital disposal of babies varies with location but may include: cremation with medical waste before transport to a landfill, cremation with other babies with eventual burial (non-public location) and flushing into the sewer system. Babies under 20 weeks may be classified as medical waste or biohazard waste. This varies by state and by hospital. This is a hard truth, but it is better to know what you may be facing. People are working to change this.
[When I delivered my second lost baby, Andrew, I prepared a birth plan ahead of time that included everything I did and did not want done. I also discussed these things with my doctor before the date of induction. When I arrived at the hospital I gave the staff the birth plan (they made a copy and gave me the original) and discussed our wishes. We agreed on everything before the induction began. There is a separate page with some specific suggestions concerning the birth plan and what I did at the hospital to ensure I would be able to take my baby home.]
If you want to reassure the medical personnel, bring photographs (on your digital camera or phone) that you have taken of the baby. When I went to the doctor’s office for an exam and ultrasound the day after I delivered Innocent, I brought photographs of him. Not only were they able to see that I had indeed delivered a baby, but they were amazed at his beauty and detail. You can help change the medieval culture surrounding miscarriage.
